Macular degeneration: what every family with history should ask their optometrist.
AMD is partly genetic and almost entirely silent until it isn't. If your mother or father had it, here is exactly what to bring up at your next exam.
Dr. E. Aimée McBride, O.D.
·April 22, 2026·6 min read
Almost every week, a patient over fifty mentions in passing that their mother had "that thing where she couldn't read anymore." That thing is usually age-related macular degeneration, and the next ten minutes of the appointment matter more than most people realize.
AMD is the leading cause of central vision loss in adults over fifty in the United States. It is partly genetic, partly lifestyle, and almost entirely silent in its earliest, most treatable stages. The patients we worry about most are the ones who say, "Well, I see fine." So do most early AMD patients — for years.
What "family history" actually means
This is the conversation we want to have with you. Having a parent or sibling with AMD roughly doubles to triples your risk. Specific genetic variants — particularly in the CFH and ARMS2 genes — are the strongest single predictor of who progresses to advanced disease. But genetics is not destiny, and most of the variance in outcome comes from modifiable factors.
So a useful first question at your exam is not "do I have it?" but rather: given what you know about my family and my own retinas today, what is my risk over the next ten years, and what can I do about it?
Why early detection is the entire game
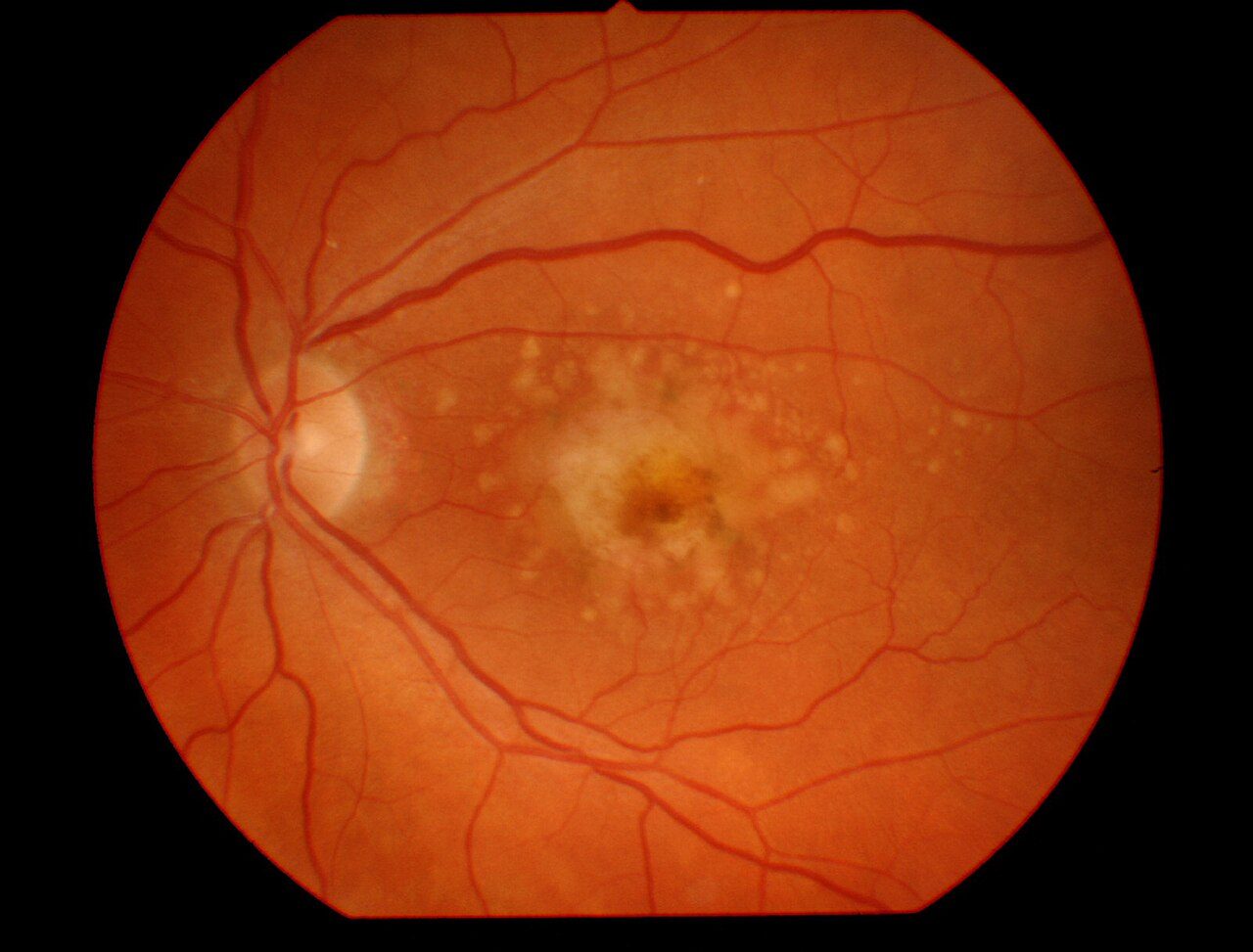
AMD has two main forms. Dry AMD is the slow form — the macula thins, small yellow deposits called drusen accumulate under the retina, and vision dims gradually. About 85% of AMD is dry. Wet AMD is the dangerous form — abnormal blood vessels grow under the retina and leak, and central vision can drop in days to weeks. Wet AMD is treatable with monthly injections (anti-VEGF drugs), and outcomes are dramatically better when treatment starts before significant scarring forms.
The math, then: catching AMD in the dry phase before it converts to wet is the single most consequential thing your eye doctor can do for you. Annual dilated exams (or Optomap imaging) make that possible.
A retinal photograph of AMD — the yellowish drusen deposits at the macula are visible years before a patient notices reading changes.
The AdaptDx test — measuring dark adaptation
Here is the test we wish every patient with family history asked us about by name. The retina contains rods (for low-light and peripheral vision) and cones (for color and detail). In AMD, the rods are damaged years before the cones — and rod damage shows up first as slowed dark adaptation, the time it takes your eyes to adjust when you walk into a dim room.
The AdaptDx® is a ten-minute, in-office test that measures this directly. It can flag AMD up to three years before any change is visible on the retinal exam itself. We use it for patients with family history, anyone over fifty-five whose retinal images show early drusen, and anyone who reports trouble adjusting to dim restaurants or driving at dusk.
The Amsler grid — at home, weekly
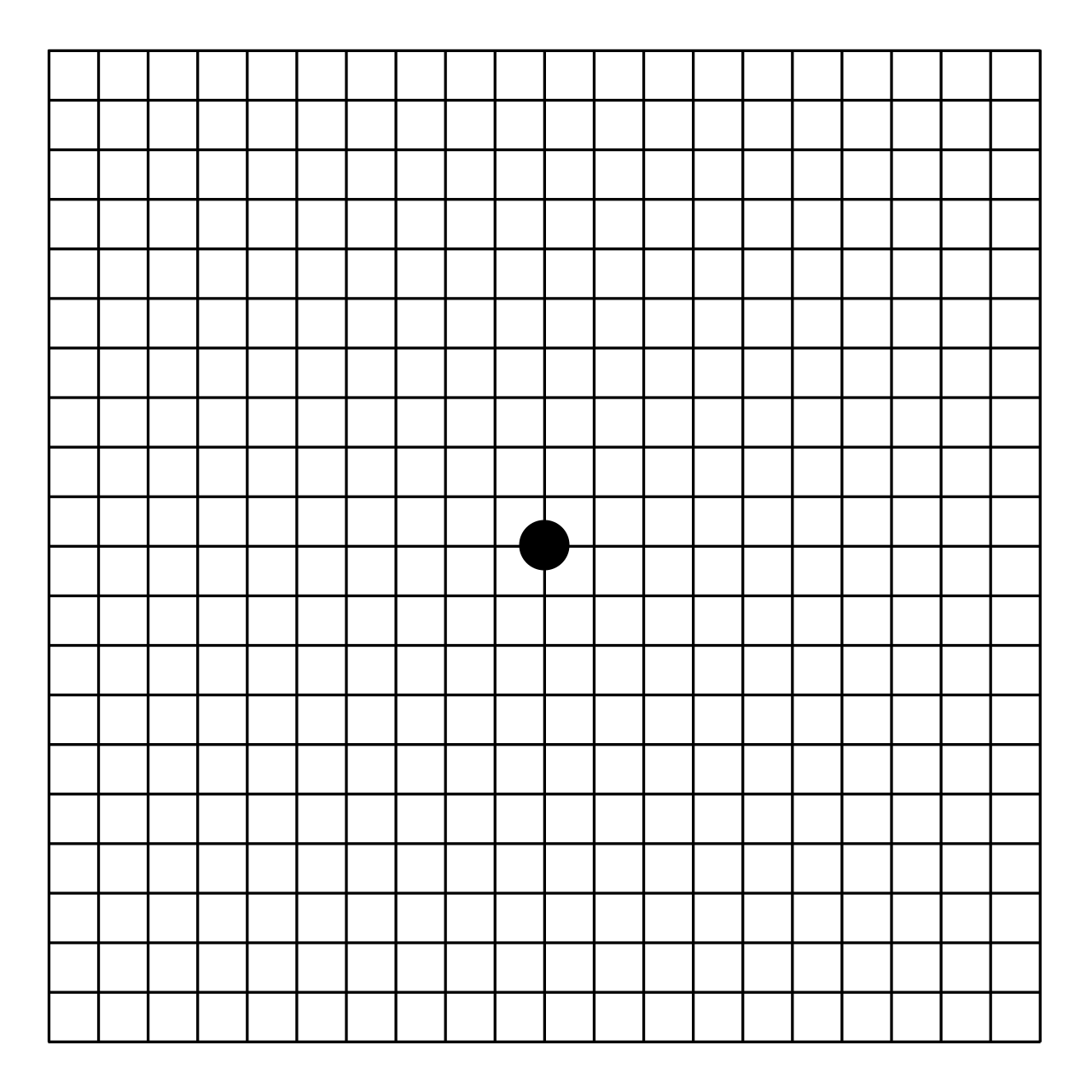
If you have any AMD risk, this is a small habit worth building. The Amsler grid is a free, paper-based home check that catches the conversion from dry to wet AMD. Look at the center dot, one eye at a time, holding the grid at normal reading distance. Any lines that look wavy, broken, or that have blank spots — that is the day to call us. Same-week appointments, always, for patients with new Amsler distortion.
The Amsler grid. Wavy or missing lines on weekly check is the symptom that buys you a same-week appointment.
What you can actually do
This is the hopeful part. Risk factors for AMD that you can modify are also among the best-studied in eye care.
Don't smoke. Smoking is the strongest modifiable risk — it roughly doubles AMD progression. If you smoke, quitting matters more for your eyes than any vitamin you can buy.
AREDS2 vitamins, if your retinas show it. The AREDS and AREDS2 trials demonstrated that a specific cocktail of lutein, zeaxanthin, vitamin C, vitamin E, zinc, and copper slows the progression of intermediate AMD to advanced disease by roughly 25%. Not a preventive — a slowing agent for the right patient. Ask us if it applies to you.
Eat dark leafy greens. Spinach, kale, collards — high in lutein and zeaxanthin, the pigments that concentrate in the macula. Twice a week, minimum.
Sunglasses outside. UV plus high-energy visible light contributes to oxidative damage in the retina. Sunglasses are cheap eye insurance. Maui Jim, Oakley, Ray-Ban — anything with proper UV blocking. Our optical can help.
Cardiovascular health. Anything good for your heart is good for the small vessels feeding your retina. Blood pressure, cholesterol, blood sugar control.
Annual exams. The cheapest, most consequential surveillance you can do. Set it up so the appointment recurs.
The questions to ask at your next exam
What do my retinal photographs and OCT scan show today?
Is there any early drusen visible? If so, where on the macula?
Should I do an AdaptDx test as a baseline?
Given my family history, what is my risk over the next ten years?
Should I be on AREDS2? If so, which brand do you trust?
How often should I check the Amsler grid at home?
Booking an exam
If you have a parent or sibling with AMD and have not been in for a comprehensive exam in the last twelve months, this is exactly what we want to see you for. Schedule online anytime, or call (828) 456-8361. Mention family history of macular degeneration so we plan the right testing into your visit. Most exams we can do same week.
About the author
Dr. E. Aimée McBride, O.D.
Dr. McBride is a co-owner of Haywood Family Eye Care. She graduated at the top of her Biosystems Engineering class at Clemson and finished her O.D. as valedictorian at UAB. Her practice focuses on ocular disease, contact lenses, pediatrics, and refractive co-management. She has provided free vision care for low-income patients and joined mission trips to Honduras.