“My endocrinologist wants me to see an eye doctor. I see fine.” We hear this every week, and it is the patient who sees fine that we are most worried about. Diabetic retinopathy is the leading cause of vision loss in working-age adults in the United States, and the cruel part is that you do not feel it coming.
The reason your endocrinologist (or your PCP) checks the box for “annual eye exam” on your diabetes checklist is not paperwork. It is one of the most important early-detection tools we have for the long-term complications of diabetes. Here is what the exam actually is, what we are looking at, and how the report gets back to your physician.
What diabetes does to your retina
High blood sugar damages the smallest blood vessels in your body. The retina is one of the most exposed places for that damage, because it is densely packed with tiny vessels that have to stay perfectly intact to feed the light-sensing cells. Over years, those vessels weaken, leak fluid and blood, and in the worst cases stop delivering oxygen to whole sections of the retina.
The disease progresses through stages we can see directly on a dilated exam or a wide-field retinal image:
- No retinopathy. The goal. Healthy vessels, healthy retina.
- Mild nonproliferative retinopathy. A few microaneurysms — tiny bulges in the vessel walls. The patient feels nothing.
- Moderate to severe nonproliferative retinopathy. More microaneurysms, small hemorrhages, patches where tiny vessels have closed off. Still mostly silent.
- Proliferative diabetic retinopathy. The retina, starved of oxygen, grows fragile new vessels. These bleed easily, scar, and can pull the retina away from the back of the eye. This is the stage where serious vision loss happens.
- Diabetic macular edema. Possible at any stage — fluid leaks into the central macula and blurs central vision. It is one of the leading causes of legal blindness in people with diabetes.
The thing to know about all of this: none of the early stages cause symptoms. Patients walk in seeing 20/20 with retinopathy already visible on imaging. That is exactly why the annual exam matters.
What the exam looks like at our office
A diabetic eye exam at Haywood Family Eye Care is a comprehensive exam with extra attention on the retina. Specifically, we will:
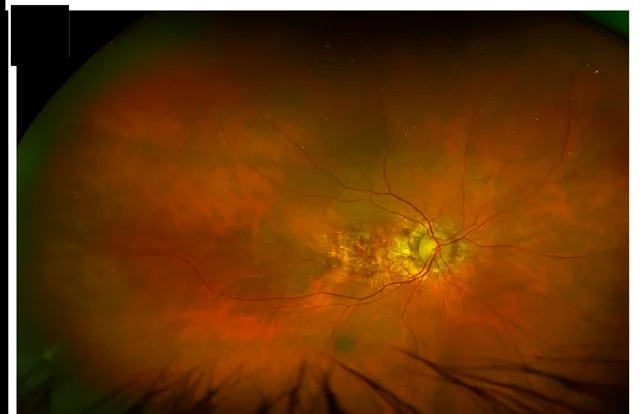
- Take ultra-widefield retinal photographs with Optomap®. A single image captures roughly 200 degrees of the back of the eye — including the peripheral retina, where diabetic changes often start — and it works through an undilated pupil.
- Dilate when it earns its keep. When the photos show anything that needs a closer, three-dimensional look, when your symptoms have changed, or when it has been more than a year since your last dilated view, we use drops and examine the retina directly.
- Scan the macula with OCT (optical coherence tomography). OCT takes cross-section images of the retina’s layers, and it is how we find the fluid that defines diabetic macular edema — often before it blurs anything.
- Compare this year to last year. Stability is what we want to see. New findings are what trigger closer follow-up or a referral to a retina specialist for treatment.
How findings get back to your physician
This part matters, and it is routine for us. With your permission, we send a written report to your endocrinologist or primary care provider after every diabetic eye exam. The report includes your visual acuity, the stage of retinopathy in each eye (if any), whether there is macular edema, a comparison to your prior exam, and our recommendation for follow-up timing — annual, six months, three months, or urgent referral.
Whether you see your diabetes doctor here in Waynesville or at one of the Asheville-area practices, just tell us at check-in who should get the report and we will make sure it lands in the right chart. Your eye exam and your A1C are two views of the same disease; the loop between us and your physician is where the exam earns its value.
What you can do between exams
How well your diabetes is managed directly affects your retina. The single best thing for your eyes is the same thing your endocrinologist is already telling you:
- Keep your A1C in your target range. Tighter blood sugar control meaningfully slows the progression of retinopathy.
- Keep blood pressure controlled. Hypertension accelerates damage to the same small vessels.
- Don’t smoke. Smoking compounds vascular damage on every front.
- Keep the annual exam on the calendar. The earlier we catch a change, the more options you have — and the more likely you keep the vision you have today.
When to call us sooner
Some symptoms should never wait for the annual visit. Call us at (828) 456-8361 the same day if you notice a sudden shower of new floaters, flashes of light, a dark curtain or shadow moving across your vision, sudden blur in one eye, or new distortion where straight lines look bent. These can signal bleeding inside the eye or a retinal problem that needs urgent attention — we will get you in, evaluate it, and if treatment is needed, arrange the retina referral immediately. Days matter with these.
About coverage
Annual diabetic eye exams are billed to your medical insurance — not your vision plan — because they evaluate a known medical condition. We work with Medicare and the major medical plans daily. Every plan handles it a little differently, so if you are unsure what to expect, call ahead and our team will help verify your benefits before the visit. No surprises is the goal.
Booking your annual exam
If you have diabetes — type 1, type 2, or gestational — and have not had a dilated or Optomap retinal exam in the last twelve months, this is exactly the appointment to make. Schedule online anytime, or call (828) 456-8361 and tell us it is a diabetic eye exam so we can plan the right testing for your visit. Diabetic eye disease is a particular clinical focus for our doctors, and it is some of the most satisfying work we do — because when it is caught early, the story almost always ends well. Let us help you keep it that way.