Almost every patient who hears the word “dilation” makes the same face. We know. The drops sting for a second, the world goes a little fuzzy, the parking-lot sun feels personal. So before we say a word about why we still recommend it, we want to say this: we hear you, and we use dilation deliberately — not by default.
That said, when we do dilate, it is because the alternative is missing things. The pupil is the only window into the back of your eye, and most of what we worry about — early glaucoma, diabetic changes, retinal tears, early macular disease, even developing cataracts in the lens itself — happens in places a small pupil hides from us. The few hours of glare are real, but they are buying you years of advance warning.
What the drops actually do
Two medications are usually involved. Tropicamide relaxes the muscle that constricts your pupil, so the pupil opens wide. Phenylephrine stimulates the muscle that pulls the pupil open, which adds a little extra room. The combination takes about twenty minutes to reach full effect and then holds the pupil open for roughly four to six hours.
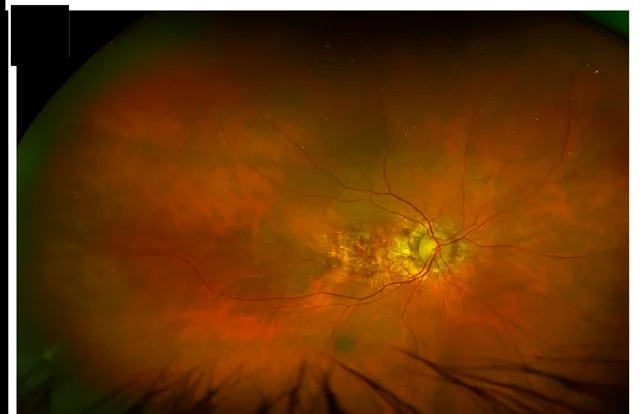
While that pupil is wide, we can look through it and see the interior of the eye in three dimensions — the optic nerve where glaucoma damage begins, the macula where age-related macular degeneration starts, the peripheral retina where tears and detachments form, and the natural lens where cataracts slowly cloud. We are looking at living tissue and the blood vessels that feed it. There is no other place in the human body where a doctor can watch small blood vessels directly, without surgery or a scan. That is also why what we see in your eyes sometimes tells us something about your blood pressure or diabetes before anything else does.
What the next four hours feel like
Honest version: not as bad as the reputation. Most patients say the worst part is the first ten minutes outside in bright sun. Here is what to expect.
- Light sensitivity. Your pupil cannot shrink to filter out bright light, so everything outdoors feels turned up. Sunglasses are essential — if you forgot yours, we’ll send you home with a disposable pair.
- Blurry near vision. The muscle that helps you focus up close is partly relaxed. Reading a menu or texting is doable but soft. Distance vision is affected much less.
- A little more glare while driving. Most patients drive themselves home comfortably, but if bright light bothers you at baseline, bring a driver or plan to wait a half hour in our waiting area before heading out. If you live up a winding road in Maggie Valley or Cataloochee, a driver is a kindness to yourself.
- Gradual wear-off. Most people are back to normal in about four hours; some patients with light-colored irises notice mild effects into the evening.
None of this is medically risky. It is a nuisance, and that is a different thing. If you have ever had a bad reaction to dilating drops, tell us — there are alternatives.
When dilation is the right call — and when it is not
We do not dilate every patient at every visit. The rule we follow: dilation matters most when the odds of finding something are highest. That includes annual exams for patients with diabetes, anyone with a family history of glaucoma or macular degeneration, patients on certain long-term medications (hydroxychloroquine, for instance, which we monitor with dedicated testing), anyone with new floaters or flashes, and the first comprehensive exam for a new patient, where we have no baseline to compare against.
For lower-risk patients, our Optomap® ultra-widefield retinal imager can often stand in for full dilation. It captures roughly 200 degrees of the retina in a single, drop-free shot through an undilated pupil, and it gives us a permanent, high-resolution image we can compare year over year — something a dilated view alone cannot do. It is excellent for most screening purposes.
It is not a full replacement for every situation. When the Optomap shows something that needs a closer, three-dimensional look, or when your risk profile points that way, we still dilate — and often the best answer is both: the wide image for the record, the dilated view for the detail. We will tell you which we recommend and why before we put anything in your eyes.
A few small things that make it easier
If a dilated exam is on the schedule, a little planning improves the rest of your day. Bring real sunglasses — the wraparound kind if you have them. If your job needs sharp near vision for the rest of the afternoon, book a late-day slot so the blur wears off at home. And if you are simply not sure whether your visit will include dilation, call and ask — we are happy to tell you in advance so nothing about the day surprises you.
When not to wait for a scheduled exam
One urgency note, because dilation is exactly how we evaluate it: if you ever notice a sudden burst of new floaters, flashes of light like a camera going off at the edge of your vision, or a shadow or curtain moving in from the side — call us at (828) 456-8361 that day. Those symptoms can mean a retinal tear or detachment, and hours matter more than days. We keep room on the schedule for urgent visits, and a dilated look at the peripheral retina is precisely how we rule the serious causes in or out.
Scheduling — and what we will explain at the visit
If it has been a year or more since your last comprehensive exam, this is what you would book. Your doctor will decide whether dilation, Optomap, or both is the right call for your eyes that visit, and walk you through why — explaining the plan clearly is how we work. Schedule online anytime, or call us at (828) 456-8361.
Dilation is a small inconvenience for what it tells us. And the Blue Ridge does not get any less pretty in fuzzy mode — promise.